Research seeds and the products and services that we aim to develop based on them
- Contents and characteristics of seeds
- Research and development results obtained so far
- R&D trends of similar competing technologies
- Ultimately aimed products and services
- Product and service analysis
1. About Seeds
- Current Status and Issues
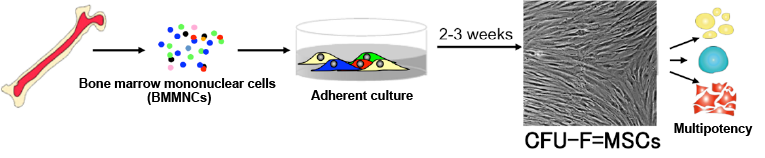
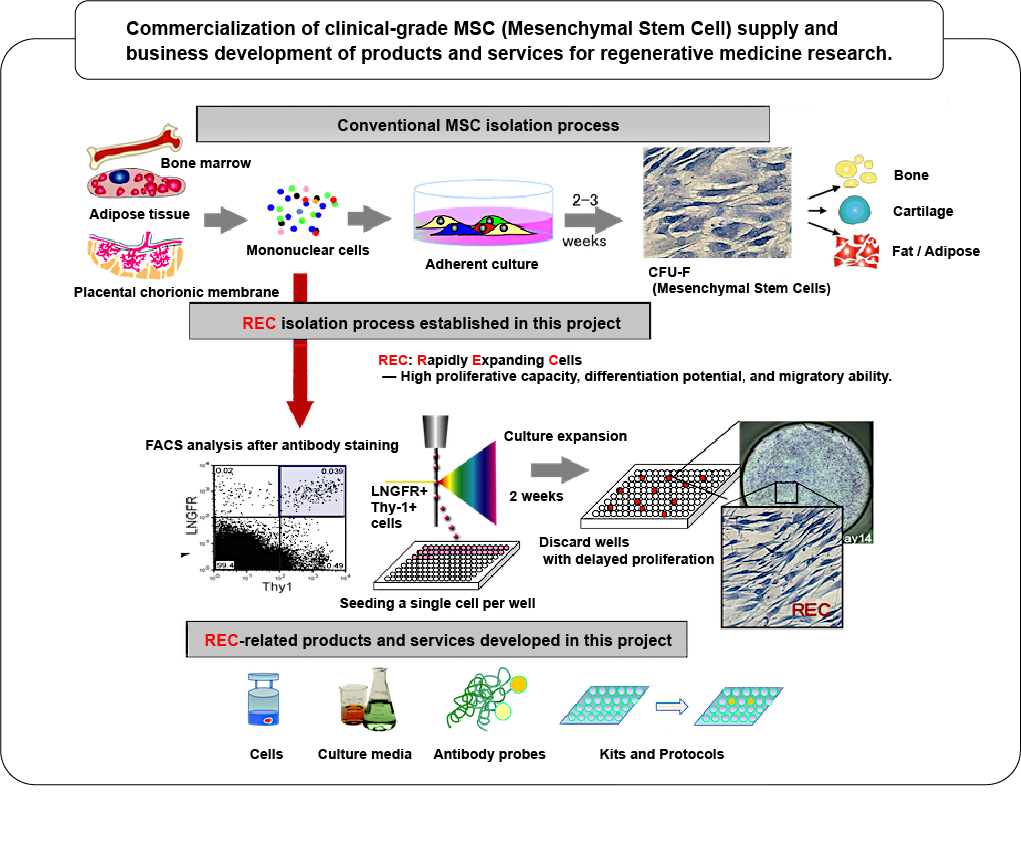
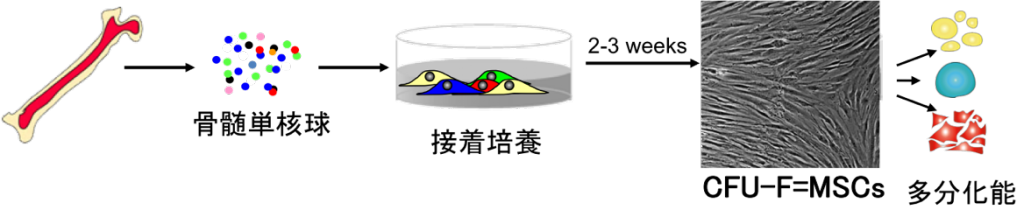
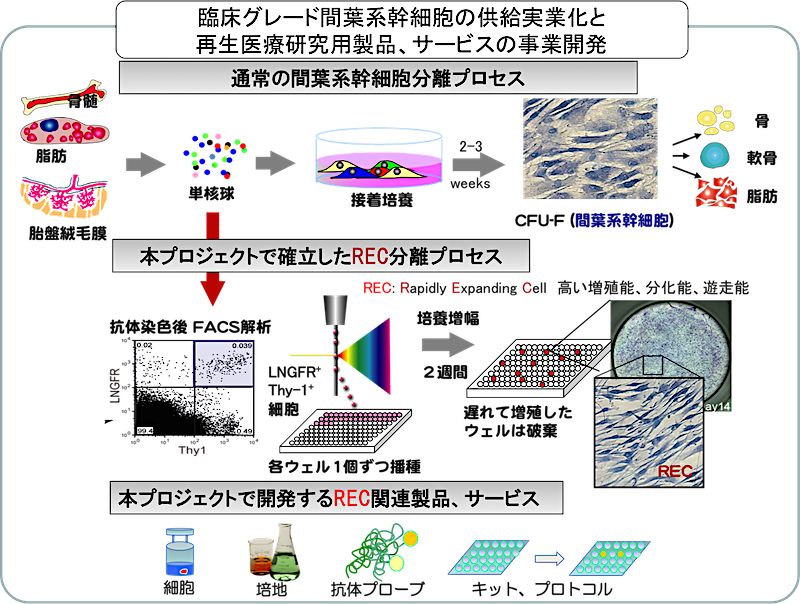
Mesenchymal stem cells (MSCs) are tissue stem cells that are expected to be the next most clinically applicable after hematopoietic stem cells because they have fewer ethical issues associated with cell collection and possess diverse differentiation potential, including bone, cartilage, and fat. Because they can be isolated using relatively simple procedures, they are widely used as biomaterials, primarily for in vitro differentiation into cartilage and bone followed by local transplantation. Investigator-initiated clinical trials have begun at several institutions. In the United States, more than 300 clinical trials are currently underway (Yano Economics Report, 2004). Currently available mesenchymal stem cells are obtained by seeding bone marrow mononuclear cells onto culture dishes and recovering the fibroblast-like colony-forming cells (CFU-F) that emerge after 2–3 weeks of culture (see figure below).
However, there are several issues with the adherent cell population obtained using this method.- Differentiation potential: Contamination with blood cells and contaminant cells with low or no differentiation potential is unavoidable, and undifferentiated cells with the ability to differentiate and proliferate (high-quality MSCs) are actually contained at a low frequency of approximately 1-3/1x103 (Colter PNAS 2000).
- Proliferation potential: MSCs, which are primary cultured cells, have a limited proliferation rate and usually lose their proliferation ability after 3-4 passages. At that time, their differentiation potential also decreases significantly.
- Migratory ability: Cell phenotypes change during culture expansion, and MSCs that maintain migratory ability within the bone marrow lose this ability during in vitro culture (Rombouts Leukemia 2003, Morikawa J.Exp.Med. 2009). For this reason, MSCs cannot be administered intravenously to treat systemic diseases.
Therefore, for safe and effective cell therapy, it is necessary to ensure the inherent cell functions of MSCs, namely, not only the proliferation and differentiation abilities that have traditionally been used as indicators, but also the uniformity and migration ability of the cells.
- Identification and Isolation of High-Quality MSCs in Human Bone Marrow
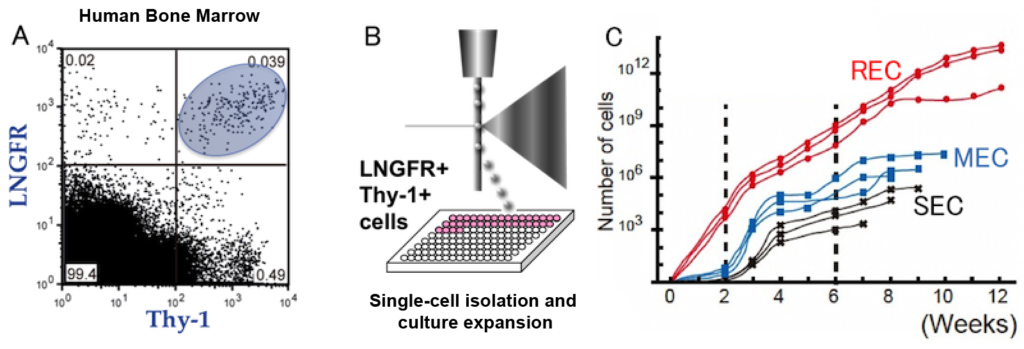
Principal Investigator Matsuzaki et al. demonstrated that the use of two antibodies, LNGFR (CD271) and Thy1 (CD90), enables highly efficient selection of human MSCs through the Ministry of Education, Culture, Sports, Science, and Technology (MEXT) Regenerative Medicine Realization Project. They then developed a technology for directly isolating human MSCs from bone marrow, peripheral blood, placental chorion, and dental pulp using a cell sorter (Mabuchi et al. Stem Cell Reports 2013). LNGFR Thy-1 co-positive cells (LT cells) form fibroblast-like colonies at an extremely high frequency of 1 in 6. Compared to whole bone marrow mononuclear cells, the colony-forming cells are enriched approximately 30,000-fold, making this the isolation method with the highest enrichment rate in the world. After these LT cells were separated into single cells in a 96-well plate (B), the proliferation rate of each well was compared, and the cells were classified into rapidly expanding clones ( REC ) that reached confluence after 2 weeks and other clones ( Medium / Slow: MEC /SEC) (C).(Rapidly Expanding Clone: REC)(Medium/Slow: MEC/SEC)(C)。
A: MSCs in human bone marrow exist in the LNGFR Thy1 co-positive fraction (LT cells).
B: Single-cell isolation of LT cells.
C: MSC clones obtained by monoculture of LT cells can be classified into three groups based on differences in proliferation rate.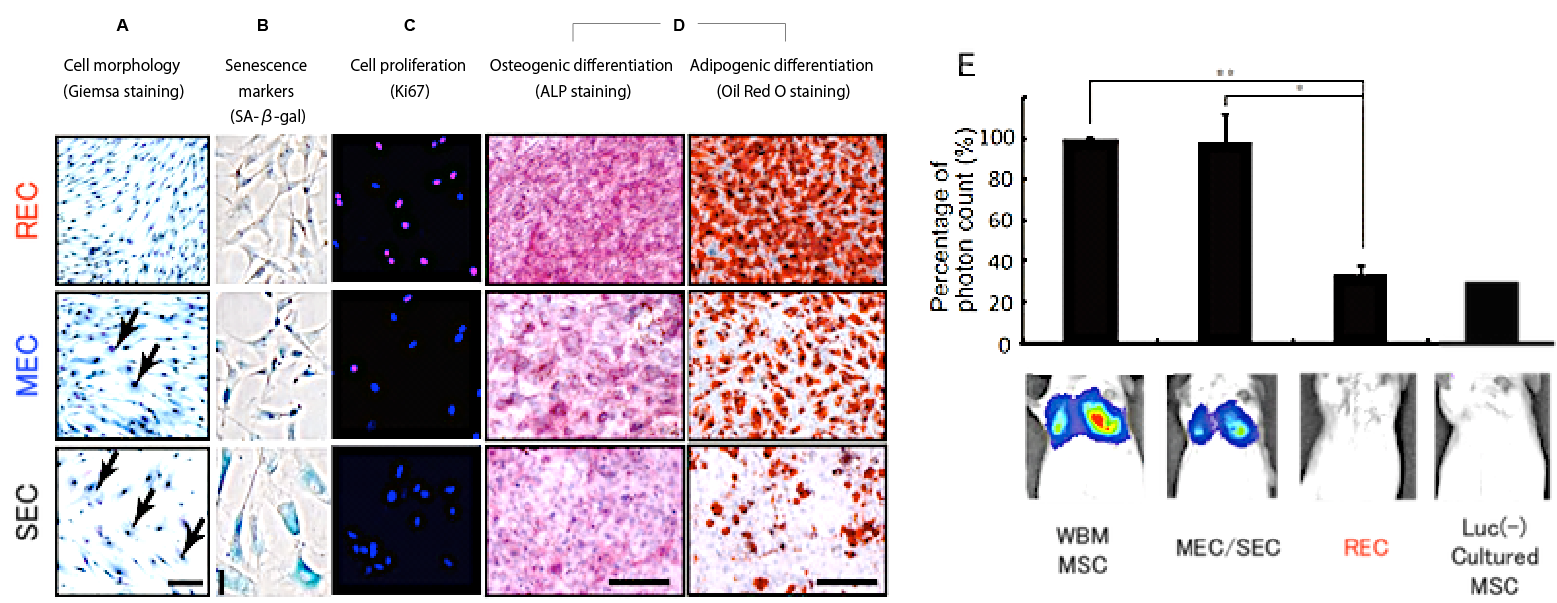
Compared to MECs /SECs,REC/ are high-quality, high-purity human MSCs that overcome all of the problems previously posed by them, including: A) they are a homogeneous cell population; B) they do not show cellular senescence; C) the majority of the cells are in the proliferation phase; D) they exhibit high differentiation potential (especially adipogenic differentiation potential); and E) they exhibit migratory properties (Mabuchi et al. Stem Cell Reports 2013).
Characteristics of REC cell performance
A: REC cell morphology is small and uniform. B: They are fresh cells that do not stain with SA-β-gal. C: The majority of RECs are positive for Ki67, a cell marker in the proliferation phase. D: Both osteogenic and adipogenic differentiation are good. E: After intravenous administration to experimental animals, no cells were observed trapped in the pulmonary capillaries. - Overview of Isolation of Highly Purified Human MSCs (RECs)
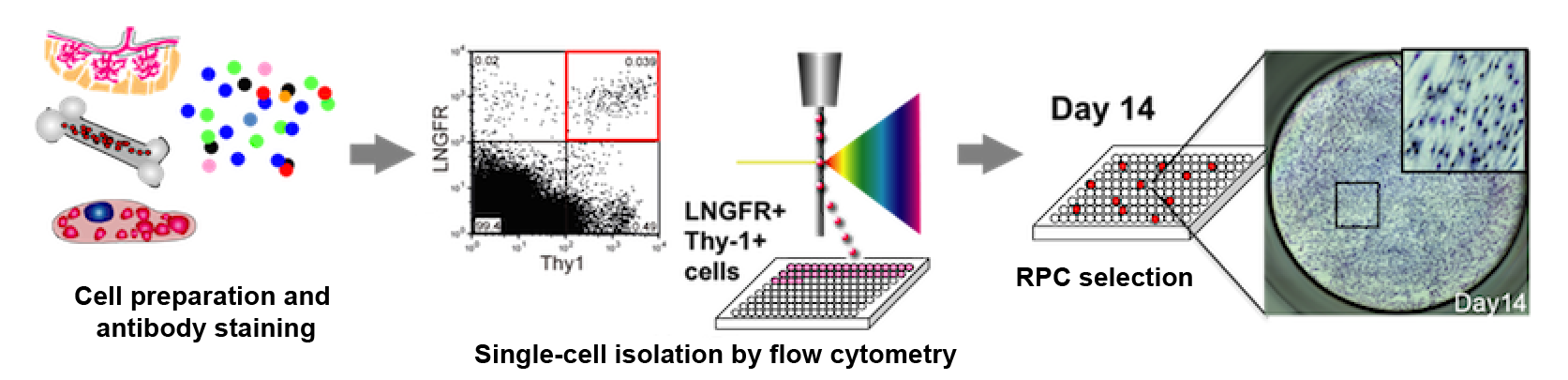
Matsuzaki et al. have demonstrated that similar cell populations can be isolated not only from bone marrow but also from adipose tissue and placental chorion. Based on these results, they established a procedure for obtaining highly purified MSCs(=REC)- Preparation of mononuclear cells from bone marrow (or fat/placental chorion)
- After staining with anti-LNGFR and Thy-1 antibodies, LT cells were single-cell sorted into 96-well plates.
- After 2 weeks, wells that reached confluence were selected (RECselection).
- Cell collection and cryopreservation
Following this protocol allows for consistent production of highly purified MSCs (Patent Application 2013-161752 / Method for Isolation and Cultivation of Human Mesenchymal Stem Cells / Matsuzaki Yumi et al. 3). Furthermore, by seeding cells recovered from one well onto a 35mm culture dish and culturing for 7-10 days, a homogenous cell population with high differentiation and proliferation potential of approximately 5x106 cells is obtained. Even after a certain period of culturing and expansion, differentiation and migration capabilities are maintained. Furthermore, the cells can be stored as frozen cells, and have already been provided to numerous research facilities as research cells. REC has an extremely high cell performance and virtually no variation between lots, resulting in an extremely favorable user reputation. Further growth is expected with its official launch on the market.
As mentioned in (1), MSCs (also known as CFU-Fs) isolated using conventional methods contain not only RECs, which have extremely high cellular activity, but also MECs/SECs, which have undergone some degree of cellular senescence (see lower figure).
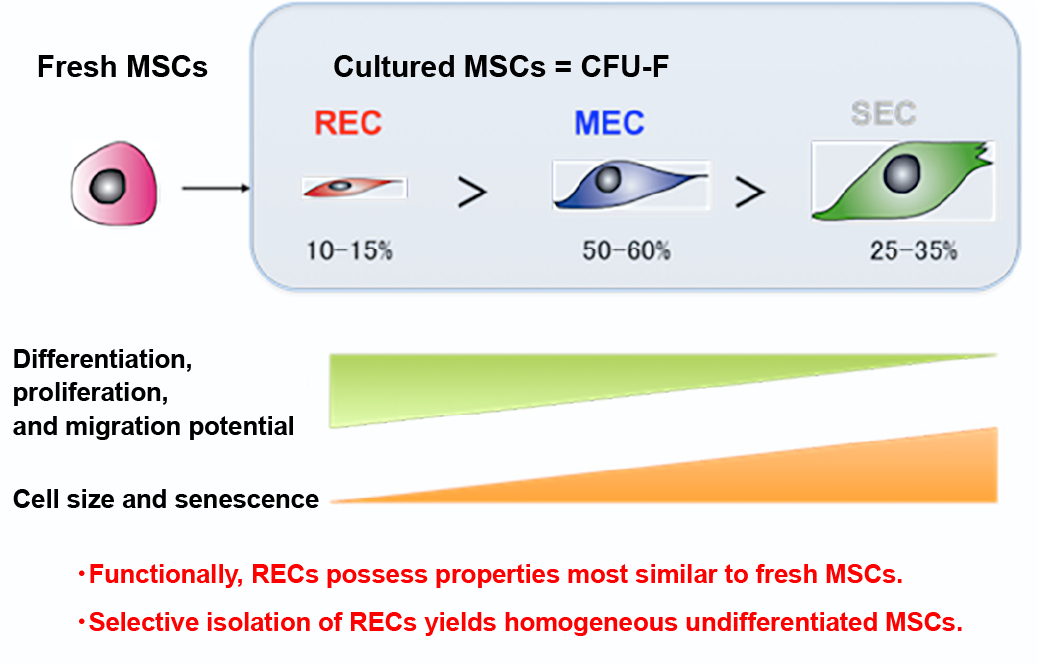
While RECs should be the only target for both research and clinical use, isolating RECs requires the single-cell isolation and clonal culture techniques established by the principal investigators. Single-cell isolation using a cell sorter is a highly specialized technique and has not yet become widely adopted. Therefore, we recognized the urgent need to develop markers that specifically recognize RECs and their corresponding antibodies, and conducted the following research and development.
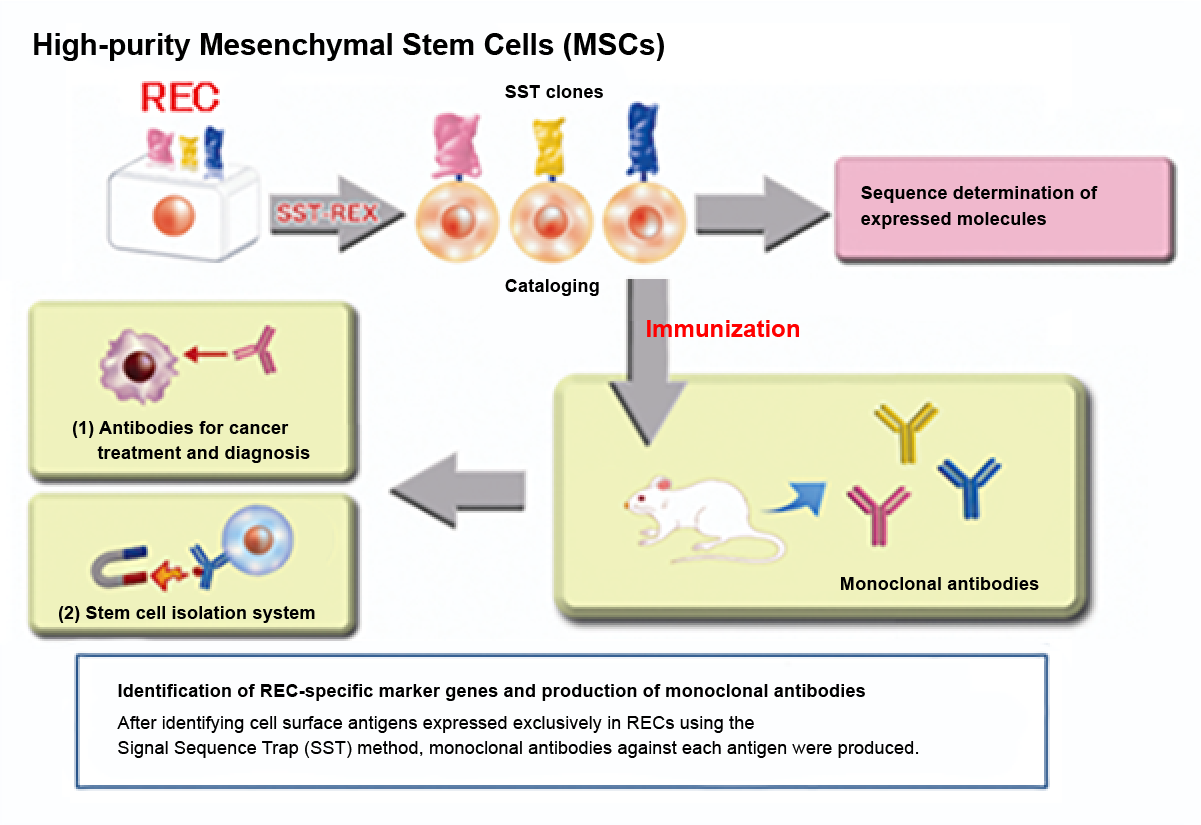
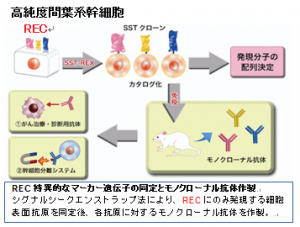
Medical and Biological Laboratories Co., Ltd. (formerly ACTGen Co., Ltd.; merged with ACTGen in March 2013) possesses a patented technology (signal sequence trap method, see lower figure) that comprehensively identifies membrane protein and secretory protein genes from any cell sample and develops monoclonal antibodies against them. This technology not only allows us to obtain genetic information on cell surface markers, but also enables the continuous development of candidate monoclonal antibodies for cell separation, which is our ultimate goal. In an industry-academia collaboration project (JST manifestation stage) that aims to further develop the technological seeds of the principal investigators into results of great significance for industrial application, we identified RECs-specific membrane proteins and produced monoclonal antibodies for five of them (lower figure).
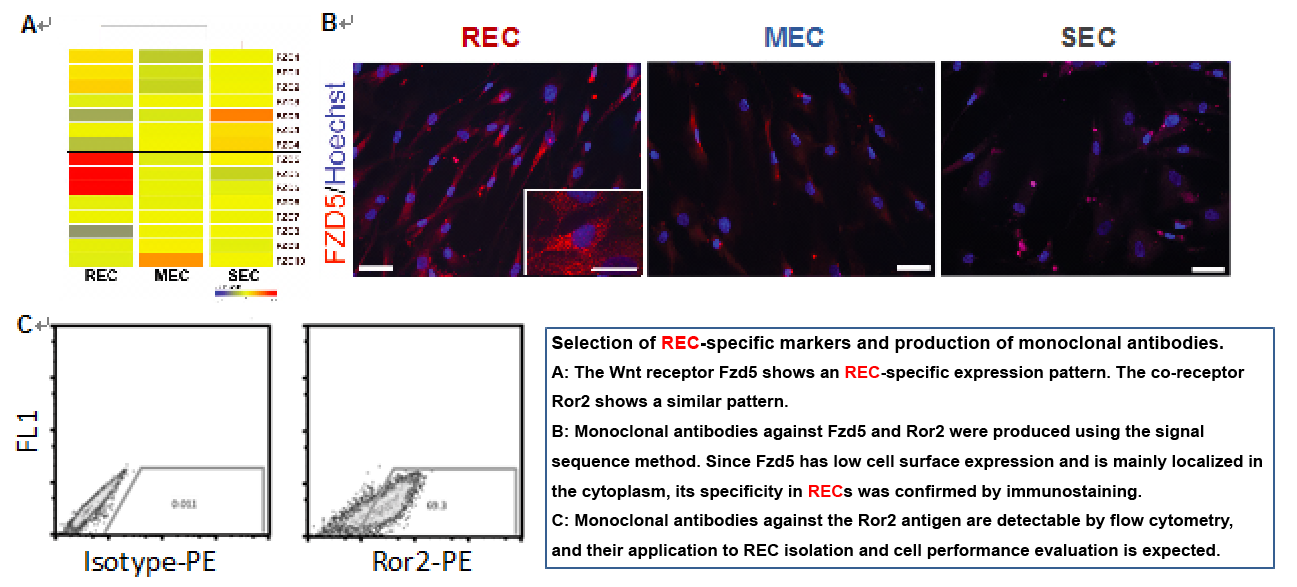
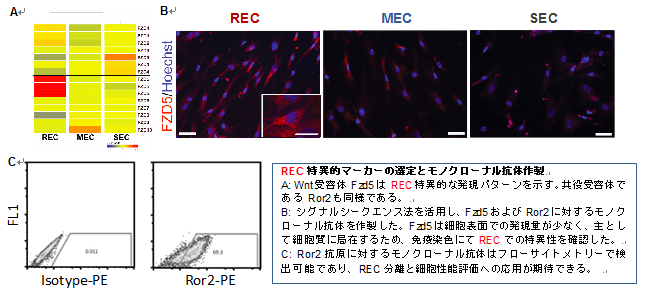
In additional studies after the manifestation stage, functional analysis of Fzd5 and its co-receptor Ror2 was completed, confirming that they are proteins essential for the undifferentiated state of RECs and that their expression is REC-specific (lower figure).
- Human bone marrow-derived MSCs obtained by conventional methods As mentioned above, currently commercially available human MSCs are cell populations obtained by conventional adherent culture, and most of the cells contained in frozen vials have low differentiation potential, divide slowly, and can only divide a limited number of times. Furthermore, it is well known that output varies depending on culture conditions and individual techniques, making it difficult to ensure reproducibility for clinical application.
- Human adipose tissue-derived MSCs
have recently attracted attention as cells that exhibit properties similar to human bone marrow-derived MSCs, and frozen vials similar to those of bone marrow-derived MSCs are beginning to be distributed. However, like the bone marrow-derived MSCs mentioned above, the isolation method used for these cells results in a cell population that is culture-isolated and contains many impurities. Furthermore, while these cells have superior adipocyte differentiation potential compared to bone marrow-derived MSCs, they have lower bone and cartilage differentiation potential, which is expected to limit their applications. - Muse cells
Muse cells are cells obtained by culturing bone marrow mononuclear cells into cell masses called M-clusters, and are said to have the ability to differentiate across germ layers, similar to ES/iPS cells (Kuroda, PNAS, 2010). Although their differentiation potential surpasses that of human bone marrow-derived MSCs, M-clusters have extremely low proliferation rate and do not proliferate at all, making it expected to be difficult to secure sufficient numbers of cells for clinical use.
Characteristics of REC cell performance (proliferation)
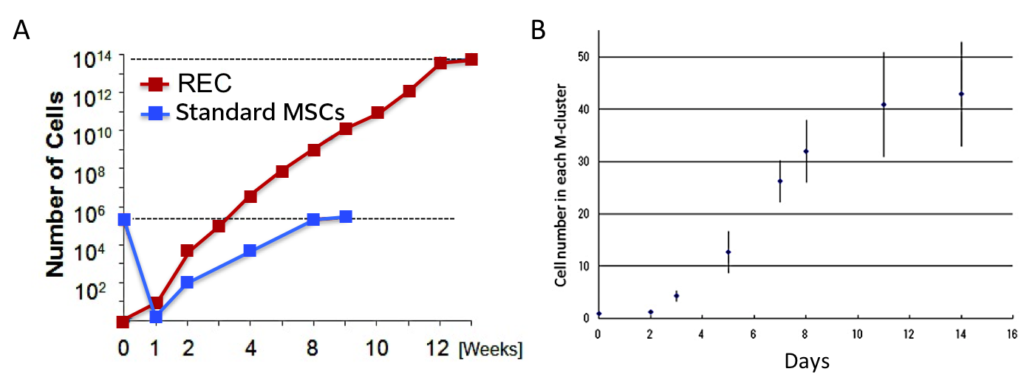
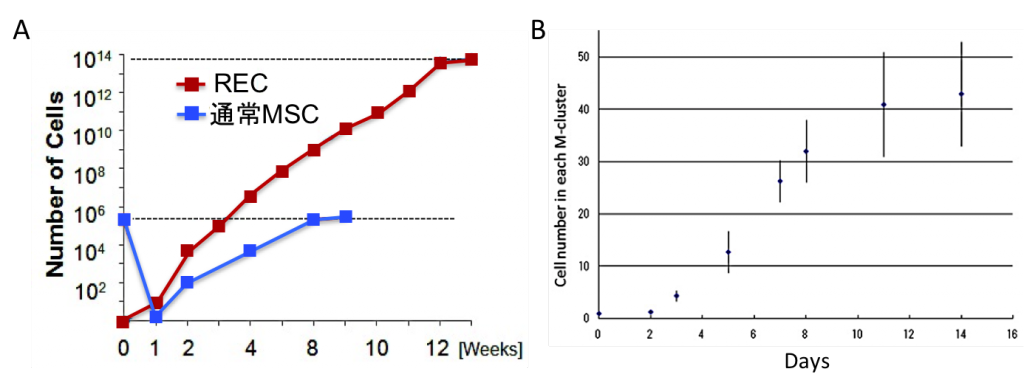
A: RECs are a cell population with extremely high proliferation potential, and one REC can be cultured and expanded to 1x1012 cells. Compared to MSCs obtained by conventional methods from the same number of bone marrow mononuclear cells, 1x106 times the cell number can be obtained. B: The proliferation potential of Muse cells contained in M-clusters is extremely low, and proliferation stops after two weeks, meaning that the maximum number of Muse cells that can be obtained from one cell is 40 (from PNAS 2010). - Pluripotent stem cell (ESC/iPSC)-derived MSCs
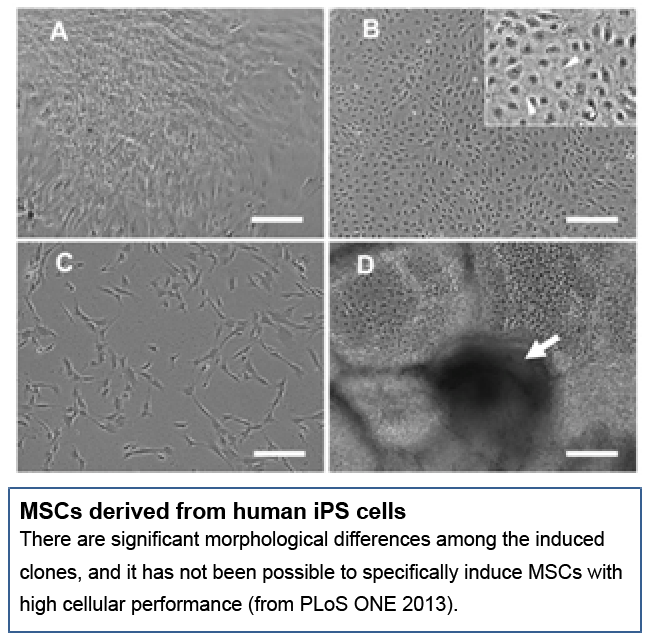
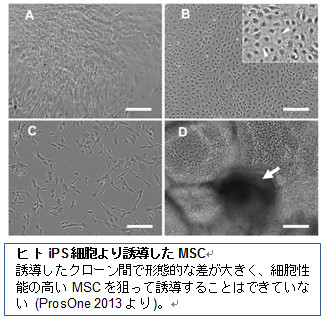
Several reports have been published on MSCs derived from pluripotent stem cells (ES cells/iPS cells) (Giuliani Blood 2011, Liu ProsOne 2013). However, as with isolation from bone marrow mononuclear cells, a homogenous cell population with excellent differentiation, proliferation, and migration properties has not yet been obtained. Furthermore, the number of days required for induction, isolation, and culture is longer than that required for isolation from bone marrow mononuclear cells. Furthermore, the risk of contamination with undifferentiated cells and the resulting risk of teratoma formation has not yet been eliminated. While promising, this approach is currently not practical.
2. Contents of products and services based on the seeds
- Commercialization of frozen vials of high-purity mesenchymal stem cells and establishment of a contract service.
High-purity mesenchymal stem cells purified using the cell separation technology originally developed by Matsuzaki et al. will be sealed in frozen vials and commercialized as mesenchymal stem cell products for research use. Furthermore, with a view to adapting them to transplantation medicine, we will establish a system to ensure stable supply of high-purity stem cells with guaranteed cell performance and GMP-compliant levels, build a clinical-grade high-purity MSC separation system, and provide contract cell separation and culture services to clinical facilities. - Mesenchymal stem cell isolation and evaluation reagents, cell culture reagents
Among the monoclonal antibodies specifically staining high-purity mesenchymal stem cells newly developed during the manifestation stage, candidates suitable for cell separation are bound to nanomagnetic particles and commercialized as mesenchymal stem cell isolation reagents. Furthermore, cell evaluation reagents are required to verify the quality of isolated mesenchymal stem cells. We commercialize fluorescent-conjugated antibodies and cell staining reagents as reagents for evaluating the cell quality of mesenchymal stem cells for transplantation. Furthermore, because mesenchymal stem cells require a stable culture environment for their self-proliferation and differentiation capabilities when applied to medical applications, we also offer optimized cell culture reagents.
- High-Purity Mesenchymal Stem Cells
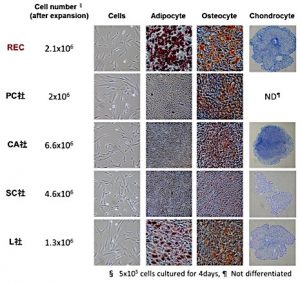
As mentioned above, mesenchymal stem cell transplantation has already been applied clinically. However, the cells isolated using existing methods only contain 0.1-1% stem cells, leaving purity an issue. According to the "Domestic Mesenchymal Stem Cell-Related Regenerative Medicine Market Forecast (Yano Research Institute, Ltd.: 2004)," the regenerative medicine market is expected to reach 112,000 cases in 2010 and 218,720 cases in 2015. As developed countries continue to age, the number of patients is expected to continue to increase. Furthermore, the regenerative medicine market in the United States is estimated to grow to 600 billion yen by 2020, and the social and economic impact of regenerative medicine using highly purified mesenchymal stem cells is expected to be significant. The figure on the right presents some data comparing image025four currently commercially available products (frozen human bone marrow-derived MSCs) with RECs . When 5 x 106 cells were cultured for four days, RECs achieved average results, ranking third out of five in terms of cell proliferation rate. However, the top-ranked cells, CA and SC, lacked the ability to differentiate into fat cells and lacked full multi-differentiation potential. Furthermore, PC cells, which had a proliferation rate comparable to RECs cells, only possessed the ability to differentiate into bone. As such, human bone marrow-derived MSCs on the market vary in proliferation and differentiation ability, resulting in significant quality differences between lots and products, which can affect experimental accuracy and reproducibility when used in research. Clinically, they lack consistency in terms of therapeutic efficacy. We believe that bringing RECs to market will offer significant advantages, as it overcomes all of the challenges posed by currently widely used MSC cells. - ClinicalRECContract Service
The enactment of the Act on the Safety of Regenerative Medicine, etc., which allows medical institutions to outsource the culturing and processing of cells for regenerative medicine, has made it easier to develop contract services by establishing facilities and procedures that comply with safety standards for cell culturing and processing. Clinical facilities, such as university hospitals, isolate RECs from bone marrow (or placental chorion/adipose tissue) collected from patients , expand them under GMP-compliant culture conditions, and use them in clinical research for transplantation therapy. Research results are shared with the clinical facilities receiving the supplies, and know-how on cell quality control, quality evaluation, and quality standard setting is accumulated, which will be utilized in future clinical development toward pharmaceutical approval as a regenerative medicine product. AIST, which has already achieved clinical MSC isolation, has completed technology transfer of cell culture procedures and other know-how within the CPC to the Shimane University Hospital Transfusion Department, establishing GMP-level culture operations and procedures for conventional MSCs using an isolator installed within the university hospital. Through this project, the goal is to establish a closed-system RECs isolation procedure and operate the facility as a contract facility. - Antibodies for Mesenchymal Stem Cell Quality Assessment
Unlike conventional small molecule drugs, cell therapy, which uses cells derived from tissue donors that vary from batch to batch, is recognized as challenging to standardize. The inability to identify the main component by physicochemical means, such as a specific molecular weight or structural formula, is the most significant difference between cells and small molecule drugs when considering formulation standardization. Because the main component of cell therapy is the cells themselves, standardization is crucial due to factors such as donor origin and the influence of the manufacturing process. Therefore, the development of markers that can be used to produce mesenchymal stem cells of a uniform grade is urgently needed, especially regarding gene expression, which directly correlates with clinical efficacy. CD markers are used as one definition of mesenchymal stem cells. By incorporating functional markers essential for cell function into manufacturing and release testing standards, combined with CD markers, standardization of cell functionality becomes possible. To this end, we believe that the monoclonal antibodies we have developed against a group of genes involved in maintaining the undifferentiated state of MSCs are highly promising.
研究シーズとそれを基に目指す製品・サービスの内容
1.シーズについて
- 現状と問題点
間葉系幹細胞は細胞採取に伴う倫理的問題が少なく、骨・軟骨・脂肪などへの多様な分化能を持つことから、造血幹細胞に次いで臨床応用が期待されている組織幹細胞である。比較的簡単な手技により分離できることから、主に試験管内で軟骨・骨などへ分化誘導後に局所へ移植するなど、バイオマテリアルの材料として広く用いられ、いくつかの施設では臨床治験が医師主導型で開始されている。また米国では300件以上の臨床試験が行われている(2004年矢野経済報告書より)。
現在流通している間葉系幹細胞は、骨髄単核細胞を培養皿上に播種し、2~3週間培養後に出現する繊維芽細胞様のコロニー形成細胞(CFU-F)を回収するという方法で得る(上図)。
しかしこの手法で得た付着細胞集団にはいくつかの問題がある。- 分化能:血球細胞や分化能が低いもしくは完全に失った夾雑細胞の混入が避けられず、実際に分化・増殖能を持つ未分化細胞(高品質MSC)は約1-3/1x103 という低頻度でしか含まれていない (Colter PNAS 2000)。
- 増殖能:初代培養細胞であるMSCは増殖回数に限界があり、通常は3-4回のパッセージ後には増殖性を失う。またその際、分化能も著しく低下している。
- 遊走能:培養増幅中に細胞の形質変化が起こり、骨髄内では遊走性を維持していたMSCが試験管内で培養するうちにその遊走性を失ってしまう(Rombouts Leukemia 2003, Morikawa J.Exp.Med. 2009)ため、経静脈投与による全身性疾患治療用途には使用不可である。
従って、安全かつ効果的な細胞治療のためには、MSCが本来持つはずの細胞機能、すなわち従来から指標とされてきた増殖能と分化能のみでなく、細胞の均一性や遊走能を保証する必要がある。
- ヒト骨髄に存在する高品質MSCの同定と分離方法開発
研究責任者の松崎らは文部科学省・再生医療の実現化プロジェクトを通じてLNGFR (CD271) Thy1 (CD90)の2種の抗体を用いることで極めて効率よくヒトMSCを選別することができることを明らかにし、骨髄・末梢血・胎盤絨毛膜・歯髄からセルソータを用いてヒトMSCを直接分離する技術を開発した(Mabuchi et al. Stem Cell Reports 2013)。
LNGFR Thy-1共陽性細胞(以下LT細胞)は6個中1個という極めて高頻度で線維芽細胞様コロニーを形成する。全骨髄単核細胞と比較し約3万倍のコロニー形成細胞が濃縮されており、世界で最も高い濃縮率を達成した分離方法である。
このLT細胞を96穴プレートに単一細胞分離後(B)に各ウェルの増殖速度を比較すると、2週間後にコンフルエントになる増殖が速いクローン(Rapidly Expanding Clone: REC)と、それ以外(Medium/Slow: MEC/SEC)に分類される(C)。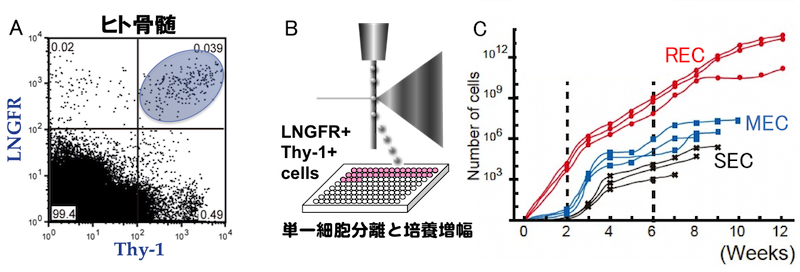
A: ヒト骨髄中のMSCはLNGFR Thy1共陽性分画(LT細胞)に存在する。
B: LT細胞の単一細胞分離。
C: LT細胞を単一培養して得たMSCクローンは増殖速度の差によって3つのグループに分類できる。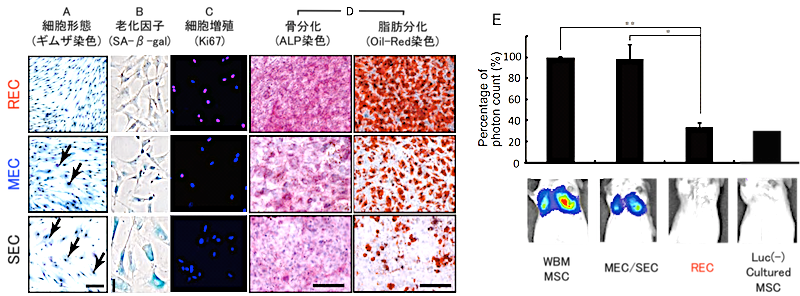
RECはMEC/SECと比較し、A) 均一な細胞集団である、B)細胞老化を示していない、C) 細胞の大部分が増殖期にある、D) 高い分化能(特に脂肪分化能)を示す、E) 遊走性を示すなど、これまで問題となっている点をすべてクリアした高品質かつ高純度なヒトMSCと言える (Mabuchi et al. Stem Cell Reports 2013)。
RECの細胞性能の特長
A: RECの細胞形態はサイズが小さく均一である。B: SA-β-galで染色されない新鮮な細胞である。C: RECの大部分が増殖期にある細胞マーカーであるKi67陽性である。D: 骨分化・脂肪分化共に良好である。E: 実験動物への経静脈投与後、肺毛細血管に補足された細胞が認められない。 - 高純度ヒトMSC(REC)の分離概要
松崎らは骨髄のみならず脂肪組織および胎盤絨毛膜より同様の細胞集団を分離できることも明らかにしている。以上の結果を基に高純度MSC(=REC)を得る手順を確立した。- 骨髄(または脂肪・胎盤絨毛膜)より単核細胞を調製
- 抗LNGFRとThy-1抗体で染色後LT細胞を96穴プレートに単一細胞ソーティング
- 2週間後にコンフルエントになったwellを選別(RECの選別)
- 細胞の回収と凍結保存
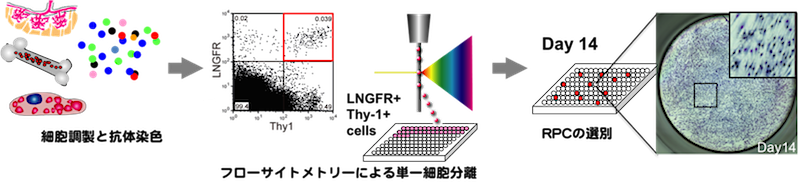
このプロトコルに準ずれば安定して高純度MSCが得られる(特願 2013-161752/ヒト間葉系幹細胞の分離培養法/松崎有未他3名)。さらに1 wellから回収した細胞を35mm培養皿に播種し7-10日間培養増幅すると、約5x106個の高い分化増殖能を持つ均一な細胞集団が得られる。一定期間の培養増幅後も分化・遊走能は維持されている。また、凍結細胞として保存が可能であり、研究用細胞としてすでに多数の研究施設に供与した実績を持つ。RECは細胞性能が極めて高く、ロット間の差がほぼ見られないことからユーザーの評判は非常に良好であり、正式に上市することで更なる発展が見込まれる。
(1) で述べたように、従来法で分離したMSC(CFU-Fとも呼ばれる)には、細胞性能の極めて高いRECだけでなく、やや細胞老化が進んだMEC/SECが混在している(下図)。
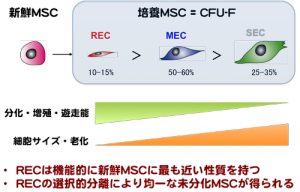
研究用・臨床用いずれもRECのみを対象とすべきであるが、RECのみを分離するには、研究責任者らが確立した単一細胞分離とクローン培養によらざるを得ない。セルソータによる単一細胞分離手技は専門性の高い技術であり、一般的に普及するにはいたらなかった。そこでRECを特異的に認識するマーカーとそれに対する抗体の作製が急務と考え以下の研究開発を行った。
株式会社医学生物学研究所(旧株式会社ACTGen:2013年3月に合併)は、任意の細胞サンプルから膜蛋白質および分泌蛋白質遺伝子を網羅的に同定し、それらに対するモノクローナル抗体開発を行う特許技術(シグナルシークエンストラップ法:下図)を有している。本技術は細胞表面マーカーの遺伝子情報を得るだけでなく、最終目標である細胞分離用のモノクローナル抗体候補の連続的な開発も可能とするもので、研究責任者らの技術シーズを更に産業応用上意義の大きい成果に育てる産学連携プロジェクト(JST 顕在化ステージ)において、REC特異的な膜蛋白質の同定を行い、その内5種類についてモノクローナル抗体作製を行った(下図)。
顕在化ステージ終了後の追加検討において、Fzd5およびその共役受容体Ror2について機能解析が完了し、RECの未分化性に必須の蛋白であること、発現がREC特異的であることなどが確認できている(下図)。
- 通常法で得たヒト骨髄由来MSC
現在商用に流通しているヒトMSCは、前述のように従来法である付着培養によって得られた細胞集団であり、凍結バイアル中に含まれる細胞のうちほとんどの細胞は分化能が低く、分裂速度が遅い上に分裂できる回数も限られている。また、培養条件、個々の手技によってはアウトプットにばらつきがでることはよく知られており、臨床応用に供する上で再現性を確保することが困難であることが大きな問題となっている。 - ヒト脂肪組織由来MSC
最近、ヒト骨髄由来MSCに近似した性質を示す細胞として、ヒト脂肪組織由来MSCが注目されており、骨髄由来と同様な凍結バイアルが流通しつつある。しかしその分離手法は上記骨髄由来MSCと同様、培養分離した夾雑物の多い細胞集団である上、骨髄由来MSCと比較し脂肪分化能に優れる反面、骨・軟骨分化能が低く、その用途が限られることが予想される。 - Muse細胞
Muse細胞は骨髄単核細胞をM-clusterと呼ばれる細胞塊状に培養して得た細胞であり、ES/iPS細胞同様に胚葉を超えた分化能を示すとされる(Kuroda, PNAS, 2010)。分化能の面ではヒト骨髄由来MSCを凌駕するが、反面、M-clusterの増殖性は極めて低く、ほぼ増殖しないため臨床に供するに足る細胞数の確保が困難であることが予想される。
RECの細胞性能の特長(増殖性)
A: RECは増殖性が極めて高い細胞集団であり、1個のRECから1x1012個まで培養増幅が可能である。同数の骨髄単核細胞から通常法得たMSCと比較し、1x106倍の細胞数が得られる。B: M-cluster中に含まれるMuse細胞の増殖性は極めて低く、2週間目には増殖が止まってしまうため、1個の細胞から40個のMuse細胞を得るのが限界である(PNAS 2010より)。 - 万能性幹細胞(ES細胞/iPS細胞)由来MSC
ES細胞あるいはiPS細胞から誘導したMSCに関する報告がいくつかなされている(Giuliani Blood 2011, Liu ProsOne 2013)。しかしながら、骨髄単核細胞からの分離同様、分化増殖遊走性にすぐれた均一な細胞集団を得るには至っておらず、また誘導・分離・培養に要する日数は骨髄単核細胞から分離する以上に必要である。さらに、未分化細胞の混入とそれによるテラトーマ形成等の危険性は未だ払拭されておらず、将来的に有望ではあるが現在までのところ実用性に乏しい段階である。
2.シーズを基にした製品・サービスの内容
- 高純度間葉系幹細胞の凍結バイアルの製品化と受託サービスの整備
松崎らが独自に開発した細胞分離技術を用いて精製した高純度の間葉系幹細胞を凍結バイアルに封入し、研究用途の間葉系幹細胞製品として商品化する。さらに、移植医療への適合を視野に入れ、細胞性能が保証され、GMPに準拠したレベルの高純度な幹細胞を安定的に提供する体制を整備し、臨床用高純度MSC分離システムを構築し、臨床施設への細胞分離・培養受託サービスを提供する。 - 間葉系幹細胞分離用・評価用試薬、細胞培養用試薬
顕在化ステージで新規に作製した高純度間葉系幹細胞に特化した染色性を示すモノクローナル抗体のうち、細胞分離に適した候補はナノ磁気微粒子と結合させることによって、間葉系幹細胞分離用試薬として事業化する。また、分離した間葉系幹細胞の品質を検定するためには、細胞評価用の試薬が必要となる。移植用間葉系幹細胞の細胞品質評価用試薬として、蛍光物質結合抗体、細胞染色用試薬を事業化する。さらに、間葉系幹細胞を医療へ応用する際、自己増殖能と分化能を有するには安定的な培養環境が必要となる為、最適化された細胞培養用試薬もあわせて提供する。
- 高純度な間葉系幹細胞
既述したように、間葉系幹細胞移植医療は、すでに臨床応用はされているものの、既存の手法で分離された細胞は幹細胞としてはわずか0.1-1%が含まれているにすぎず、純度に課題が残る。再生医療の市場は「間葉系幹細胞関連の国内再生医療市場予測((株)矢野経済研究所:2004 年度)」によると、2010 年に112,000 件、2015 年に218,720 件と予想されている。今後、先進諸国の高齢化が進むとともに、さらに患者数が増え続けるものと考えられる。また、米国では再生医療関連の市場は2020 年には6,000億円に成長すると推定されており、高純度間葉系幹細胞を用いた再生医療への社会的貢献、社会経済への効果は大きいものと予想される。
右図に実際に現在市販されている4社の製品(凍結ヒト骨髄由来MSC)とRECを比較したデータの一部を紹介する。5×106 cellsの細胞を4日間培養した際、RECは、細胞の増殖速度では、5細胞中3番目と普通の成績であるが、上位に位置するCA社とSC社は脂肪への分化能がなく、完全なるマルチ分化能を有していない。また、REC細胞と同等の増殖率であるPC社の細胞は、骨への分化能しか有していなかった。このように、市場に流通しているヒト骨髄由来MSCは増殖能や分化能が様々で、ロット間・製品間の品質の差が大きく、研究に供する場合には実験精度および再現性に影響を及ぼす。臨床的に見た場合、治療効果の面で安定性に欠ける。RECを市場に乗せることは、現在広く使われているMSC細胞の課題を全て克服できるため、優位性が高いものと考えている。 - 臨床用REC受託サービス
医療機関が再生医療用細胞の培養加工を外部に委託するのを認める「再生医療等安全性確保法」の施行により、細胞の培養加工について定める安全基準に適合する施設や作業手順を整えることで、受託サービスの展開が容易になった。大学病院などの臨床施設が患者から採取した骨髄(あるいは胎盤絨毛膜・脂肪組織)よりRECを分離後、GMPに準拠した培養条件で増幅し、移植治療の臨床研究に活用してもらう。供給先の臨床施設と研究成果を共有し、細胞の品質管理や品質評価、品質規格の設定に関するノウハウを蓄積し、再生医療製品として薬事承認に向けた今後の臨床開発に生かす。すでに臨床用MSCの分離実績を持つ産総研よりCPC内での細胞培養手順その他のノウハウは島根大学病院輸血部へ技術移転が完了しており、大学病院内に設置されたアイソレーターによるGMPレベルでの通常MSCの培養操作と手順は確立されている。本プロジェクトを通じて閉鎖系でのREC分離手順を確立することで、受託施設として稼働させることを目標にする。 - 間葉系幹細胞の品質評価用抗体
従来の低分子医薬とは異なり、製造バッチごとに異なる組織提供者(ドナー)に由来する細胞を用いる細胞医療においては、製剤の規格化が困難であることが認識されている。特定の分子量、特定の構造式といった物理化学的な手段でその主製剤の特定ができないことが、製剤の規格化を考える上で、細胞と低分子薬で最も大きな相違点である。細胞医薬は細胞自体が主製剤であるため、ドナーに由来する違い、製造工程の影響を受けるなどの面から、規格化が極めて重要となる。したがって、間葉系幹細胞を均質なグレードで製造するための指標となるマーカーの開発は急務であり、臨床効果に直結する遺伝子発現については特に管理が必要となる。間葉系幹細胞の定義の1つとしてCDマーカーが利用されているが、それらと組み合わせて、細胞機能に必須の機能性マーカーを製造工程や出荷試験の規格に導入することで、細胞の機能性の規格化が可能となる。この目的に対し、申請者らが作製したMSCの未分化性維持に関わる遺伝子群に対するモノクローナル抗体は極めて有望と考えている。